

Abstract
Background: Diffuse large B-cell lymphoma (DLBCL) and Burkitt lymphoma (BL) are aggressive lymphomas that evolve rapidly and are fatal if untreated. Most treatment-related toxicities occur during the initial phase of therapy, particularly in the elderly and in patients with a high disease burden. Prephase therapy is used as a preventive strategy prior to definitive multiagent chemotherapy to ameliorate the development of toxicity, such as febrile neutropenia, tumor lysis syndrome, deterioration in performance status, and death. While this approach is often implemented, there are few data supporting when to initiate a prephase regimen, or whether this approach will be effective. We present data from our experience at the University of North Carolina Cancer Hospital.
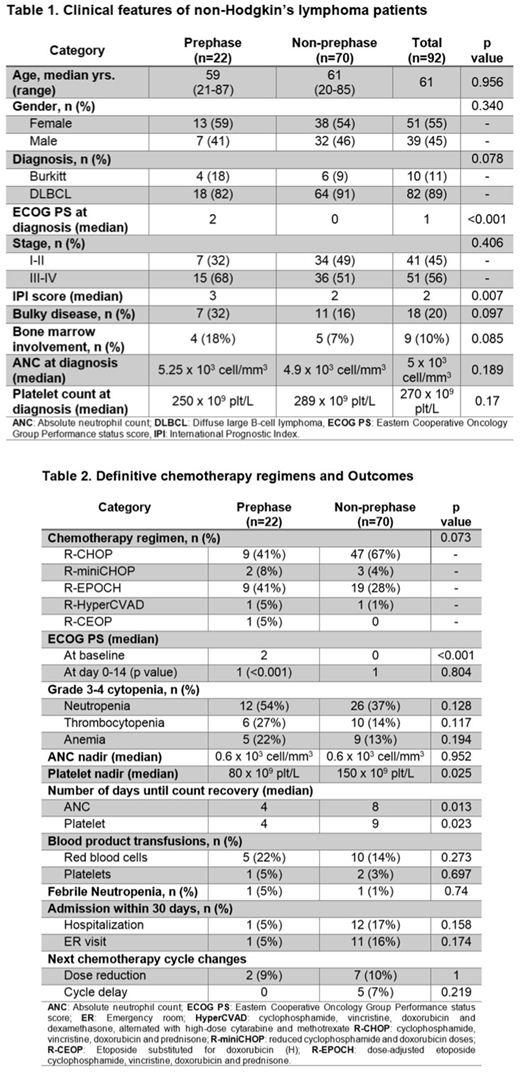
Methods: We conducted a retrospective analysis of patients (pts) diagnosed with DLBCL and BL between January 2016 and December 2017. Pts were divided into 'prephase' (PP) and 'non-prephase' (NPP) groups. The PP group received either prednisone (P) alone at 60 mg/kg oral daily from day -6 to day -1, or in combination with vincristine (V) 1 mg intravenously on day -6 (VP regimen), cyclophosphamide 200 mg/m2 on day -6 (CP regimen), or all three drugs (CVP regimen). Multiagent chemotherapy was given at day 0. Both groups were evaluated until day 30. ECOG performance status (PS), grade 3-4 cytopenias, absolute neutrophil count (ANC) and platelet nadirs, time to ANC and platelet recovery, episodes of febrile neutropenia, hospitalization and emergency (ER) visits, and next cycle dose reduction or delay, were compared in both groups.
Results: Ninety-two pts (DLBCL n=82, and BL n=10) were identified. Clinical characteristics are shown in Table 1. Twenty-two pts received PP therapy (vs. NPP n=70). Median age at diagnosis was 59 years and 61 years for PP and NPP group, respectively. Female predominance was observed in both groups (PP 59% and NPP 54%). Poor baseline ECOG PS was significantly different between the PP and NPP group (median score 2 vs. 0, p<0.001). Stage III-IV and bulky disease were more common in the PP group, although this was not statistically significant. Oral prednisone was the most common prephase therapy used (P n=17, VP n=1, CP n=1, CVP n=3). All regimens were well tolerated. Definitive chemotherapy regimens and outcomes are summarized in Table 2. The PP group had a significant improvement in PS from a median PS of 2 at baseline to a median PS of 1 (p<0.001) by day 14. The NPP group did not have a significant change in PS. In a subgroup analysis, both pts older than 60 years with any PS (n=10, p=0.027), and pts 60 years or younger with a PS of 2 or more (n=6, p=0.023) had a significant improvement in PS after prephase therapy. PP pts had a shorter time for ANC and platelet count recovery than NPP pts (ANC 4 vs. 8 days, p=0.013; platelet 4 vs. 9 days, p=0.023). The platelet nadir was significantly lower in the PP (80 x 109 plt/L) compared to the NPP group (150 x 109 plt/L) (p=0.025). There was no significant difference in the episodes of febrile neutropenia.
Conclusions: Prephase therapy significantly improved PS by day 14 of definitive multiagent chemotherapy at first cycle. The overall improvement in PS was primarily caused by improvements in 2 groups: pts older than 60 years, and pts 60 years or younger with poor PS (ECOG PS 2 or more). This is consistent with who we would expect to benefit the most from prephase therapy. Patients who received prephase therapy had a significant reduction in the length of their ANC nadir, although, interestingly, the rate of febrile neutropenia was low in both arms. The length of the platelet nadir was also significantly reduced in the PP group. Conversely, the depth of platelet nadir was significantly lower in the PP group, which may be a reflection of more aggressive disease in this group. The prephase group trended towards a reduction in the number of hospital admissions, ER visits, and next cycle dose reduction or delays, but these did not reach statistical significance. Based on these results, we will implement a provider reminder to consider prephase therapy when using multiagent chemotherapy in pts with aggressive lymphomas older than 60 years, or pts <60 with PS of 2 or greater.
Grover:Seattle Genetics: Consultancy. Dittus:Seattle Genetics: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal